
As a patient going through IVF, you likely interact with your doctor and the nursing staff a lot. There are consultations, blood tests, follow-ups, and ultrasounds that lead up to egg retrieval. Once the egg retrieval is performed, it’s a matter of weeks until you go back into the office for the embryo transfer. After the retrieval it may seem like your doctor “takes it from there”. In actuality, the eggs are handed off to a team of highly trained embryologists that perform the actual IVF and other procedures. We sat down with embryologist Evelyn E. Neuber, Ph.D., HCLD (ABB), Clinical Research Coordinator at the Center for Advanced Reproductive Services at UCONN to get the inside scoop on the life of an embryologist.
This interview was conducted by Shannon Wieloch.
How did you decide to become an embryologist?
When I was 22, I took a Reproductive Biology class at Boston College and had the opportunity to look in a microscope and see a fertilized human egg for the first time. It took my breath away. I remember thinking this is the coolest thing I have ever seen. I could not stop talking about it all day. Eventually, my roommate asked “Why don’t you just become an embryologist then?” So I did!
What kind of education did you pursue to become an embryologist?
I started on a general biology track during my undergrad at Muhlenberg College, a small liberal arts school in Allentown, PA and then went on to Boston College to get my Masters and PhD.
So you need a PhD to be an embryologist?
Embryologists don’t need a PhD, or even a Master’s; the minimum requirement is a Bachelor’s degree, typically in biology. However, becoming an embryologist is less about earning a specific degree and more about on-the-job training. Most IVF labs have a stepwise program of advancement to senior embryologist: at UCONN you start by spending a year doing data entry and observation, then you assist in setting up equipment. Eventually embryologists work up to practicing on mouse embryos and learning how to handle human embryos with a technique called micromanipulation, which allows you to make the super small movements that are necessary when dealing with such delicate cells. Other techniques that are taught on the road towards becoming a senior embryologist include egg retrieval, intracytoplasmic sperm injection (ICSI), embryo biopsy, and embryo vitrification (freezing).
In addition to on-the-job training, the embryologists at UCONN go to various meetings and host guest lecturers to help us stay up to date on the latest IVF laboratory techniques and procedures.
So, is this the route you took, then — working your way up the ranks at UCONN?
Actually, my embryology training began at Boston IVF, when I was a graduate student and continued through my post-doctoral education. Then I spent a few year at Yale University both doing research and working in the IVF laboratory. It was there that I completed the training and received my High-Compliance Clinical Laboratory Director (HCLD) certification. So the short answer is, I came fully-baked to UCONN! So much so that they made me an Instructor in the Department of Obstetrics and Gynecology at the University of Connecticut School of Medicine.
Wow! That’s an impressive resume! Can you tell us more about what embryologists actually do?
There are four main procedures that an embryologist assists with or performs directly: egg retrieval, ICSI, embryo biopsy and vitrification, and embryo transfer.
Egg retrieval and embryo transfer are relatively straightforward from the embryologist’s perspective: during egg retrieval, a doctor collects follicular fluid containing an egg from a patient’s ovary and then hands it to the embryologist who is responsible for isolating the egg from the liquid and preparing it for insemination with the sperm; during embryo transfer, the embryologist loads the embryo onto the catheter and hands it to the MD who does the actual transfer. However, it’s the parts in between these steps – ICSI and biopsy – that I think are the most exciting.
Can you explain what is involved with ICSI?
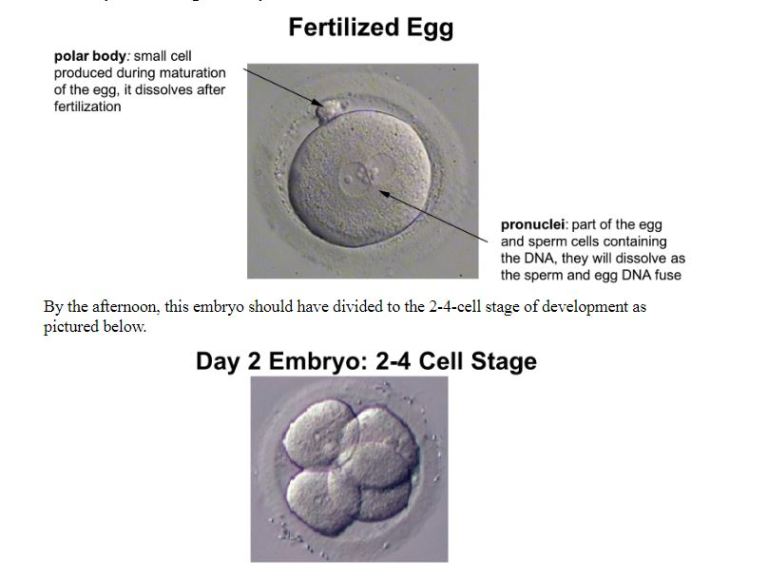
During ICSI, the embryologist uses micromanipulation tools to inject a single sperm into the egg and then continues to monitor the embryo’s development over the next five days. The picture below shows an egg (16-18 hours after ICSI) that has undergone normal fertilization and is well on its way to becoming an embryo.
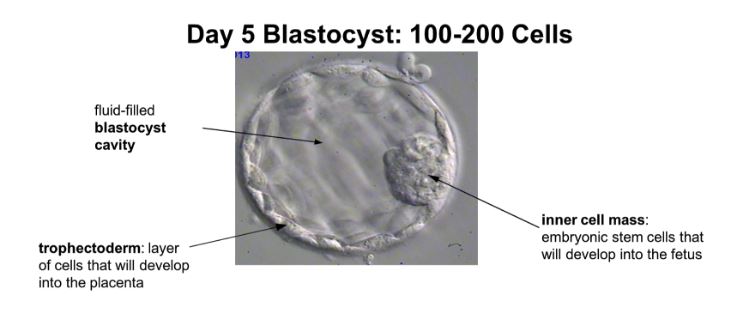
By 5 days, the embryo should be approximately 100-200 cells and is termed a blastocyst. It is at this stage that an embryo can be biopsied for genetic testing and/or vitrified (frozen) for later use.
What is involved in embryo biopsies?
At UCONN, senior embryologists perform the more complex procedures like embryo biopsies and vitrification. Training for biopsy and vitrification includes practice on mouse embryos or abnormal human embryos that were donated for research, followed by sharing cases under the direction of a more experienced embryologist. Some preimplantation genetic testing (PGT) companies also work with embryologists to develop their biopsy technique; embryologists can send in samples to verify the amount of cells and quality of the sample submitted. This is critical. The goal is to remove 5-10 cells from the trophectoderm, the part of the developing embryo that will become the placenta (see below). In real clinical cases, these cells undergo preimplantation genetic screening (PGS) to determine if an embryo has the appropriate amount of chromosomes and is likely to lead to a successful pregnancy.
What is vitrification and why is it done?
After biopsy, an embryo is vitrified, i.e., quickly frozen, using liquid nitrogen. This prevents ice crystal formation so the embryos can be safely stored in tanks of liquid nitrogen until they are needed.
Do all clinics have that intense kind of biopsy training?
I hope so! If you are going to do PGS, I recommend going to a clinic whose embryologists perform biopsy regularly. It is a skill, and technique is everything.
Is there a “typical” work day?
There is definitely no typical day when dealing with patients, but there is a general and consistent workflow.
My day begins with quality control (QC) for the entire lab. One of the biggest challenges is the rigor of the QC that is performed in all IVF labs. When I first started my career, it felt as if we just checked that the machines were plugged in. Now, before anything is opened, moved, or set-up, I verify and document countless QC measurements, including the room temperature, the pH of the media used to grow the embryos, lot numbers of reagents, microscope temperature settings, and gas tank levels. Only when I am 100% certain that everything is in optimal working order do I open the IVF lab for business.
After QC, I look at the eggs that were retrieved the day before to assess for signs of fertilization (they will look like the fertilized egg picture above if everything was successful). Next, I prep for any embryo transfers scheduled for that day by verifying that a given embryo is at the right stage of development. If it is not, we must postpone that patient’s procedure for another day. Egg retrievals come next followed by actually performing all of the embryo transfers that have been given the green light earlier in the day. Finally, I enter the “Patient Free Zone”, where it is just me and the samples, and perform all of the core embryology techniques – cleaning eggs, ICSI, biopsies, and freezing.
What is the best part of your job?
ICSI is my favorite thing to do. It is such a cool and satisfying procedure because you get results (in this case, hopefully a successful fertilization) the next day, which is not typical for science. The injection of a single sperm into a mature egg requires time to perfect, but it gets easier with experience.
What is the hardest part of your job?
The most difficult aspect of my job is the pressure of it. I get vested in patients and their outcomes, so I feel terrible in the cases where it doesn’t work out and thrilled when it does. On the same lines, because I know how high the stakes are, I am constantly focused on what I am doing. I have to be meticulous all the time. My job requires extreme focus and continuous double checking (though a second embryologist has to check everything too, which takes some of the pressure off).
How do you unwind at the end of a hard day?
I’m busy with my kids and my home life. And I’ve recently rediscovered tennis. Though on tough days, a glass of wine always helps!
What are some of the biggest changes to the world of IVF in your 25-year career?
Oh my! Well for starters we used to make and hand deliver our own media for the embryos via the Boston subway system! Today clinics typically purchase the media and have it delivered.
How do you think PGS and PGD have changed the fertility landscape?
I think both are incredible advancements. To think that with PGD, somebody with a family history of a genetic condition can do something about it- it’s amazing. Though the field is advancing so quickly that sometimes we have new information before we even feel like we know what to do with it – like in the case of mosaic PGS results.
Is there anything I didn’t specifically ask that you want our readers to know?
Teamwork is very important. It’s not just one person doing this. It’s a team effort. If I’m not on, than another embryologist is. Every day counts and it’s important that everything is done the same. We’re a large center with six to seven embryologists so we have standardized protocols that enable someone to step in and continue the process. Someone is always there.
Perhaps your baby was conceived with Evelyn’s help, or perhaps it will be in the future. For anyone undergoing IVF, it’s guaranteed that an embryologist somewhere, at some time, will be a part of the team that makes your miracle happen.
