
Mosaicism continues to be highly discussed in the ART community. Despite several recent studies looking at what happens after a mosaic embryo is transferred,1,2 there are still plenty of unanswered questions.
What is chromosomal mosaicism?
First and foremost, it’s important to understand what chromosomes and mosaicism are:
What are chromosomes?
Think of our DNA as a long string. To fit all of our DNA into a cell, the DNA is tightly wound into structures called chromosomes. We typically have 23 pairs of chromosomes, for a total of 46 chromosomes.
What is mosaicism?
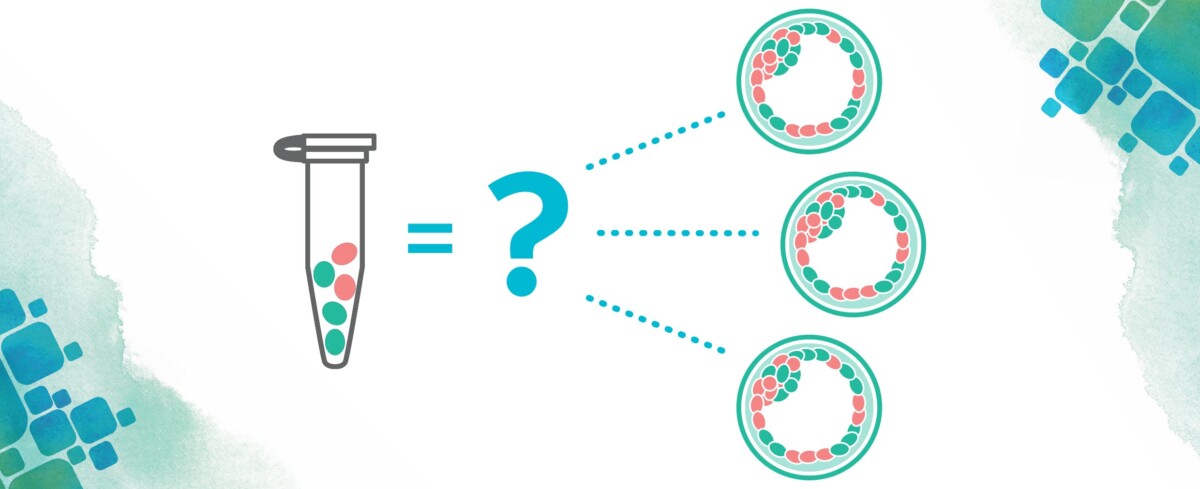
Mosaicism describes an embryo sample with two or more chromosomally different sets of cells. The cells themselves are either euploid (normal number of chromosomes) or aneuploid (abnormal number of chromosomes); it is the biopsy sample that is mosaic.
At CooperSurgical, mosaic results are further characterized as low-level mosaic or high-level mosaic. Low-level mosaicism (LLM) describes an embryo sample where a lower percentage of cells in the biopsy sample is found to be abnormal. High-level mosaicism (HLM) describes an embryo sample where a higher percentage of cells in the biopsy sample is found to be abnormal.
CooperSurgical recommends these ranges for mosaicism:
- LLM: 20-40% of sample is abnormal
- HLM: >40-80% of sample is abnormal
What does it mean when there is a mosaic PGT-A result?
As with any test, it’s important to know what it is we’re actually testing. At the time of embryo biopsy, the embryo itself has two different layers of cells. The trophectoderm (TE) is the outer cell layer of the embryo that will eventually make the supporting structures of the pregnancy, such as the placenta. The inner cell mass (ICM) is the inner cell layer of the embryo that will form the fetus. A few cells are removed from the TE for PGT-A. These cells are sent to the laboratory, and the embryo itself remains at the clinic.
When looking at PGT-A results, we presume the chromosome results we see in the biopsy sample are the same as in the ICM. For embryos that have normal or abnormal PGT-A results, it is likely the ICM is either normal or abnormal. For mosaic PGT-A results, making predictions about the ICM is not as straightforward.1
When we see mosaicism in the biopsy sample, it is possible the ICM could be normal, abnormal, or also mosaic. No current technology can determine what is happening throughout either the TE or the ICM.
What do we know about mosaic PGT-A results?
If mosaic PGT-A results can’t tell us for certain what is occurring in the ICM, what do we know? What’s the likelihood of a mosaic embryo resulting in successful pregnancy? Does it matter what the chromosome abnormality is? Does it matter if multiple chromosomes are involved? Thankfully, there is literature we can rely on for this information, and there are many things we do know:
- Embryos with euploid PGT-A results have the highest implantation, ongoing pregnancy, and live birth rates. They also have the lowest miscarriage rates. 1,2
- Embryos with aneuploid PGT-A results have the lowest implantation, ongoing pregnancy, and live birth rates. Aneuploid embryos also have the highest miscarriage rates.1,2
- LLM embryos have higher implantation and ongoing pregnancy rates compared to HLM embryos.2
- Embryos with mosaic segmental abnormalities have higher implantation and ongoing pregnancy rates compared to embryos with mosaic full chromosome abnormalities. A segmental abnormality is where a large piece of a chromosome is missing or duplicated. Full chromosome abnormalities include monosomy (an entire missing chromosome) or trisomy (an entire extra chromosome).2
- The more abnormalities identified, the lower the implantation rate and ongoing pregnancy rate.2
What if my embryo has one mosaic chromosome abnormality?
When there is only one mosaic chromosome abnormality, there are some cells that have the normal number of chromosomes and some cells that have an abnormal number of chromosomes.
What if my embryo has more than one mosaic chromosome abnormality?
It can mean that there are some cells that are euploid and some cells that are aneuploid. However, it could be there are no euploid cells and all the cells are aneuploid but with different chromosome abnormalities. Importantly, when there are multiple mosaic abnormalities, PGT-A cannot determine if there are any normal cells in the biopsy.
Evidence has shown that mosaic embryos may “self-correct.” While little is known about the process or frequency of embryo self-correction, it is thought that the normal cells may outcompete the abnormal cells or the abnormal cells die off. This results in mainly normal cells within the embryo. However, there have been reported instances where the mosaic chromosome abnormality has been confirmed in an ongoing pregnancy or live born child.4
What don’t we know about mosaicism?
Despite all we do know, there is still quite a bit we don’t know. One major area that is lacking is long-term outcome data. Studies have focused mainly on rates of implantation, ongoing pregnancy, and outcome at birth. But what is expected of a newborn (and what we might see at birth) is very different from what we expect of a 2-year-old, 5-year-old, and older.
This is relevant when discussing mosaic PGT-A results because even if prenatal testing is normal or a baby appears normal at birth, there may be abnormal cells in other parts of the body that might lead to later health concerns.
Genetic counseling for mosaicism
All this information can make counseling about mosaic PGT-A results difficult. We can be reassured, based on recent literature, that if a mosaic embryo results in successful pregnancy, the pregnancy or child is most likely not going to have immediate medical or developmental issues. However, there is still a possibility for these to occur. This possibility may be increased for certain chromosome abnormalities, including chromosomes 13, 18, 21, X, Y, and certain segmental anomalies. Why these in particular? Because abnormalities of these chromosomes are associated with known genetic syndromes.
In sum, there is a real possibility for a healthy baby after transferring a mosaic embryo, and a mosaic embryo may be a great choice for some couples. However, there is also the possibility of failed implantation, early miscarriage, or a baby with medical and/or developmental issues. These risks may depend in part on the abnormality present, and couples may choose not to transfer a mosaic embryo because of this. There is no “one size fits all” for mosaic PGT-A results. Discussion should be tailored and include both the potential positive outcomes as well as the uncertainties that remain.
References:
- Popovic M et al. Extended in vitro culture of human embryos demonstrates the complex nature of diagnosing chromosomal mosaicism from a single trophectoderm biopsy. Hum Reprod 2019;34(4):758-769.
- Viotti M et al. Using outcome data from one thousand mosaic embryo transfers to formulate an embryo ranking system for clinical use. Fertil Steril. 2021 May;115(5):1212-1224.
- Viotti M. Preimplantation genetic testing for chromosomal abnormalities: aneuploidy, mosaicism, and structural rearrangements. Genes (Basel). 2020;11(6):602.
- Kahraman S et al. The birth of a baby with mosaicism resulting from a known mosaic embryo transfer: a case report. Hum Reprod 2020;35(3):727-733.
